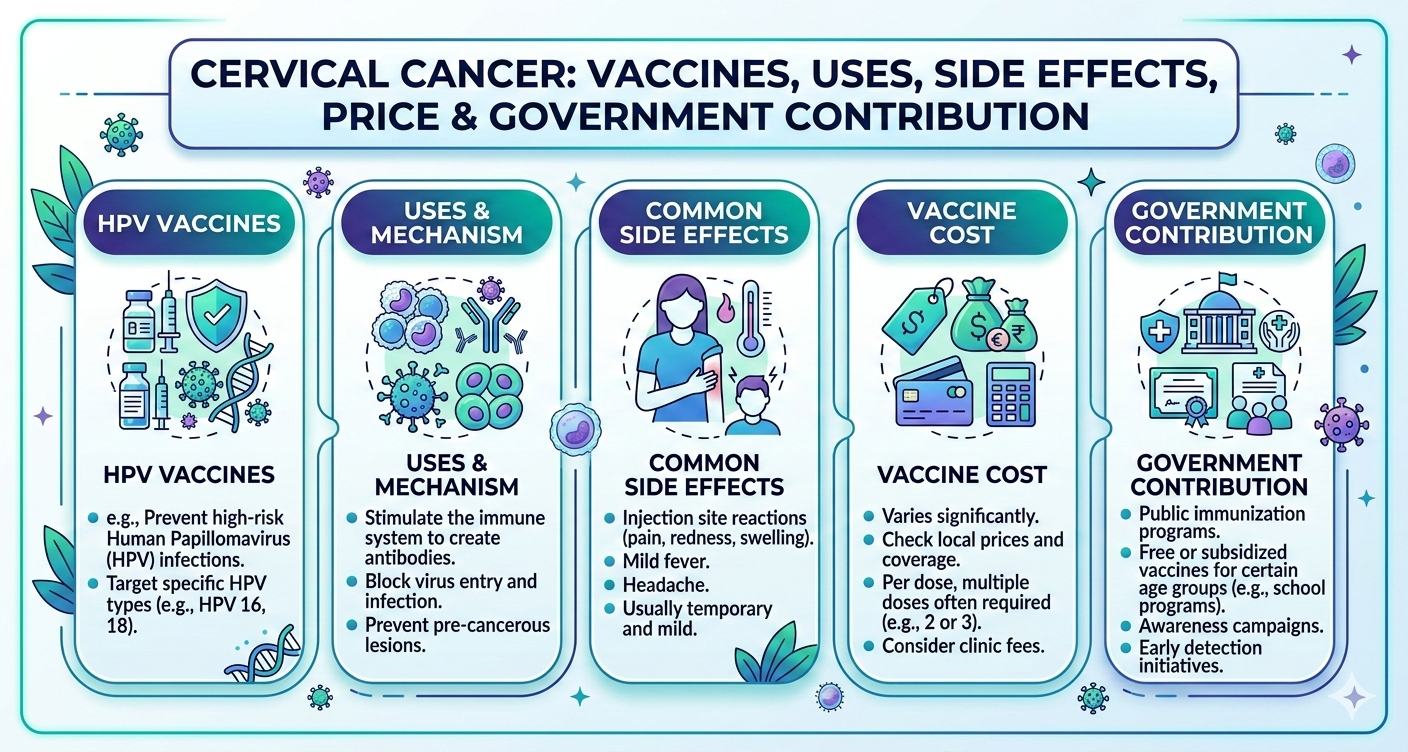
Cervical Cancer: Vaccines, Uses, Side Effects, Price & Government Contribution
सर्वाइकल कैंसर: वैक्सीन, उपयोग, दुष्प्रभाव, कीमत और सरकारी योगदान Introduction | परिचय Cervical cancer is one of the most common cancers affecting women worldwide. It develops in the cervix (the lower part of the uterus)